Early diagnosis of fetal defects
Spina bifida
In spina bifida, there is failure of closure of the neural tube with secondary damage to the exposed nerves.
- The prevalence is about 1 in 1,000 births but this is subject to large geographical variations.
- Chromosomal abnormalities, single mutant genes, and maternal diabetes mellitus or ingestion of teratogens, such as antiepileptic drugs, are implicated in about 10% of the cases. However, the precise etiology for the majority of these defects is unknown.
- When a parent or previous sibling has had a neural tube defect, the risk of recurrence is 5%.
- Periconceptual supplementation of the maternal diet with folate reduces the risk of developing spina bifida by about 75%.
Open spina bifida is associated with the Arnold-Chiari II malformation with caudal displacement of the brain stem and obliteration of the cistern magna.
In the second-trimester the sonographically detectable manifestations of the Arnold-Chiari II malformation are the lemon and banana signs.
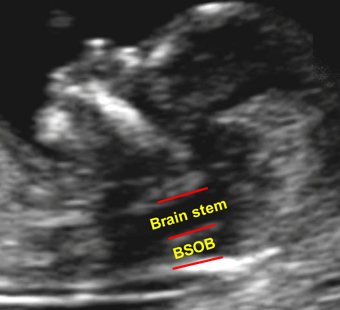
In the first-trimester the Arnold-Chiari II malformation is manifested in compression of the fourth ventricle (intracranial translucency). In the mid-sagittal view of the fetal face at 11-13 weeks the lower part of the fetal brain between the sphenoid bone anteriorly and the occipital bone posteriorly can be divided into the brain stem in the front and a combination of the fourth ventricle and cistern magna in the back. In most cases of open spina bifida the diameter of the brain stem is increased, the distance between the brain stem and the occipital bone (BSOB) is decreased and the ratio of the brain stem to BSOB is above 1.0.
Normal brain
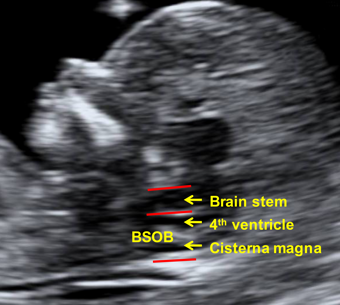
Brain in spina bifida