Background to preeclampsia
Pathogenesis
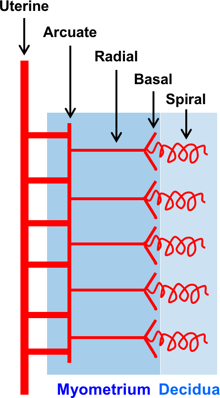
The main blood supply to the uterus is provided by the left and right uterine arteries, which branch to form, in sequence: the arcuate, radial, basal and spiral arteries.
In pregnancy, the blastocyst implants into the maternal endometrium. The outer layer of the blastocyst develops into the trophoblast, which differentiates into villous trophoblasts, which give rise to chorionic villi that transport nutrients and oxygen between the fetus and the mother and extravillous trophoblasts, which invade and transform the spiral arteries. Essentially, the trophoblasts replace the endothelial lining and destroy the musculoelastic tissue in the walls of the spiral arteries so that they are converted from tortuous narrow muscular vessels into large non-muscular channels thereby increasing maternal blood flow to the placenta.
This physiological process occurs in two stages: the first wave of trophoblastic invasion involves the spiral arteries in the decidua (endometrium of pregnancy) and starts at 8 weeks of gestation, whereas the second involves the spiral arteries in the inner third of the myometrium and occurs at 14-18 weeks.
In PE, particularly preterm PE, the physiologic process of placentation is impaired. There is trophoblastic invasion in 50-70% of spiral arteries; however, this does not extend into the myometrial segments, and is confined to the decidual part of the vessels. The spiral arteries are less dilated than the normally transformed arteries and the blood supply the placenta is reduced. The reason why in some pregnancies there is failed placentation is unknown but genetic and immunological reasons may be implicated.